



The Szaszian Fork: Another Reply to Scott Alexander on Mental Illness
On mental illness, it's either Caplan or Kirkegaard

I have a long-running debate with Scott Alexander about mental illness. I take the Szaszian view that most so-called “mental illnesses” are not illnesses at all, but socially disapproved preferences. Scott, a professional psychiatrist, says I’m deeply in error. I say Scott’s great, but deeply in error. He replies that I’m the one deeply in error. I say his marital search algorithm shows I was right all along. Neither of us has convinced the other.
Our argument is wide-ranging, but one sticking point is the fact that being gay used to officially be a mental illness, and now it’s not. Scott:
The psychiatric profession will never live down the thing about homosexuality; I fully expect that in 5000 AD someone will still be complaining that we can’t stigmatize entities infected with superintelligent self-replicating memetic viruses, because DSM-II listed homosexuality as a psychiatric disease.
Me:
Question for Scott: According to you, what do we learn about psychiatry from “the thing about homosexuality”? Do we simply learn that psychiatrists made a mistake? If so, what precisely was their mistake? After all, once you reject the distinction between preference and constraint for “anything more complicated than which brand of shampoo to buy,” why shouldn’t you label same-sex attraction as a “constraint” no different from paralysis?
Even today I bet that most gay teens would take a pill that permanently “cured” their same-sex attraction. Does that show they’re sick? If not, why not?
Scott’s original response seems uncharacteristically evasive:
We want some criteria that let us call shingles a disease, but don’t let us call “being thin but wanting to be even thinner” a disease. Unfortunately, there is no perfect solution to this problem. People have wanted perfect solutions to definitional questions ever since Plato defined man as “a featherless biped”, and it’s never worked.
This January, however, Scott wrote a piece that makes it sound like I’ve finally convinced him. Not just on being gay, but on everything. His title says it all: “You Don't Want A Purely Biological, Apolitical Taxonomy Of Mental Disorders.” Why not? Because calling a condition a “mental illness” is, as Szasz taught, rhetorical trickery. Scott:
We have to classify pedophilia as a mental illness, because we want insurance to pay for treatment. If someone shows up at a psychiatrist saying “Help, I feel an urge to molest children, is there anything you can do to get rid of that urge or prevent me from acting on it?”, I definitely want insurance to pay for this person’s treatment. Therefore, pedophilia “is” “a” “mental” “illness”, and no sophisticated categorization algorithm will ever convince me otherwise.
Am I putting my words into Scott’s mouth? Amazingly, no. Here’s Scott again:
When the DSM is political, it’s not (just) because the authors are ideologues and want to go around stigmatizing people they don’t like. It’s because “is X a mental disorder or not?” is scientifically meaningless but politically very important.*
As Eric Cartman would exclaim, “That’s what I say!”

If you follow Scott’s last link, however, you’ll discover that his actual position is more nuanced. So we haven’t yet reached a meeting of our minds:
"Disease", like "blegg", suggests that certain characteristics always come together. A rough sketch of some of the characteristics we expect in a disease might include:
1. Something caused by the sorts of thing you study in biology: proteins, bacteria, ions, viruses, genes.
2. Something involuntary and completely immune to the operations of free will
3. Something rare; the vast majority of people don't have it
4. Something unpleasant; when you have it, you want to get rid of it
5. Something discrete; a graph would show two widely separate populations, one with the disease and one without, and not a normal distribution.
6. Something commonly treated with science-y interventions like chemicals and radiation.
Scott’s even got a diagram that lets me pinpoint our disagreement in his own framework:
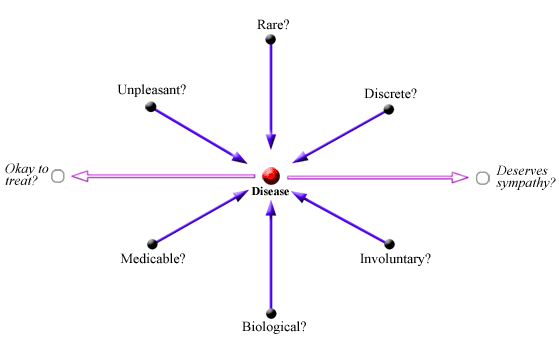
Where do I pinpoint our disagreement? I maintain that no preference is a disease. No matter how bizarre or horrible (or common or wonderful). Diseases are constraints, not preferences.
How can we tell the difference? Preferences are voluntary; constraints aren’t. “I did it because I wanted to” means voluntary. “I did it because I had to” means involuntary.
OK, how do we know what’s “voluntary” - especially in a world where people excuse bad behavior by claiming they “had no choice”? Simple: If any incentive in the universe makes you stop, you must have been able to stop all along. Incentives matter implies voluntariness implies preference implies non-disease.* That’s my Gun-to-the-Head Test.
Szaszian dogma? I call it common sense. But if you won’t bite my bullet, Emil Kirkegaard’s critique of Scott serves an alternate bullet for your culinary pleasure:
Scott doesn't want to bite the bullet and say that DSM unclassifying homosexuality was a mistake, so he has to go on complicating things about how classifications are also political, as they unlock monetary support for treatment…. I submit this is not a very, well, scientific approach. The correct solution is to recognize that homosexuality is a mental illness for the obvious reasons.
Emil’s “obvious reasons”:
Homosexuality is evolutionarily maladaptive. “From an evolutionary perspective, humans are a sexually reproducing species, so sexuality should -- must -- be targeted at the opposite sex. But furthermore, it should be targeting the right age too. So since female fertility is strongly age-dependent, men's targeting must be primarily of fecund females, so age 15-45 or so. Female targeting can be less age dependent, but should at least be 15+ (and that's what we see). Thus, if someone is targeting persons outside of the adaptive age, that is a disorder of sorts.”
Homosexuality correlates with many other heritable mental illnesses. “The most important fact about mental illness is that all the various diagnoses tend to occur together, called comorbidity. This is why one can speak of mental illness overall as a kind of trait, which we call general psychopathology, or P factor. Homosexuality relates positively to most mental problems, and for genetic reasons too.”
The stigma explanation for comorbidity is indefensible. “Stigma against homosexuals has decreased markedly in the last couple of decades, and yet homosexuals still show markedly elevated rates of mental problems. If this was caused by stigma, it should have declined rapidly, ergo, it is not caused by stigma.”
Contrary to what you’ve heard, homosexuality is treatable: “So 14 studies with a mean sample size of 25, and they used something like 14 different designs and maybe half that different measures. Ripe for publication bias and p-hacking. Still, they managed to obtain an absurdly (?) large mean effect size of 0.89 d. And some of the studies used outcomes that are not so obviously stupid such as penile volume measures. I mean, I was expecting them to just rely on self-reported sexual behavior or thoughts following extended talks with priest-therapists. It would be easy to see how social desirability bias could distort such results. So maybe, just maybe, it isn't as obviously stupid as it sounds. After all, if homosexuality can rapidly increase in the population, this suggests it can be environmentally induced, and in that case, maybe also cured (see also this post by George Francis).”
If you’re paying attention, you know that I totally disagree with Emil. And you know why. To repeat: Preferences can’t be diseases! Not alcoholism, not idleness, not the urge to commit murder, and not your sexual preferences.
Indeed, by Emil’s logic, what preferences aren’t diseases?! Being a nun or priest is evolutionarily maladaptive; it probably correlates with multiple neurotic issues even when stigma is low; and you could probably “treat” this genetically destructive occupational choice in a hundred different ways.
For that matter, the same probably goes for the preference of doing anything other than maximizing your surviving offspring. Spending money on vacations instead of kids is evolutionarily maladaptive; it probably correlates with multiple neurotic issues even when stigma is low; and you could probably “treat” this genetically destructive spending in a hundred different ways.
The punchline: Although Scott now seems a lot closer to me than I realized, he’s clinging to an unstable intermediate position on mental illness. Emil’s position may fill you with rage, but it’s logically consistent. So is mine. Choose one, because as Emil’s namesake Søren Kierkegaard titled his most famous book, it’s Either/Or.

* Yes, I person could simply have an infinitely strong preference, which would still be voluntary. Incentives don’t matter does not imply involuntariness, though it leaves the possibility open.






Tell you what, Bryan: next time I'm psychotic I'll come to your house, and we'll see how you feel about my preferences.
Remember, if you report this comment, you're not thinking like Szasz....
Is there a list somewhere of those mental illnesses you both agree are not preferences?